What is AMD?
Age-related macular degeneration (AMD) is the largest cause of registered blindness in developed countries. AMD is an age-related disease claiming 10% of the population in the age range 66-74 years, rising to 30% in those aged 75-85 years. The predicted increase in the elderly population is expected to swell these numbers. Thus the current estimate of 1.75 million sufferers in the United States is expected to grow to 3.0 million by the year 2020.
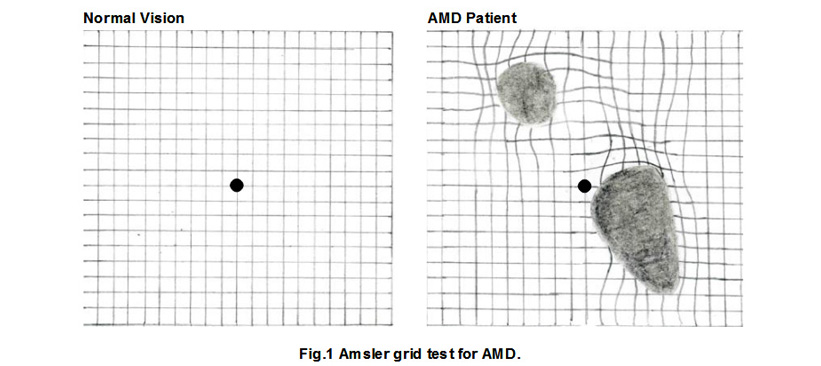
As the disease progresses, there is a gradual loss of central vision with blurring of images, missing areas within the visual field and distorted vision such that straight lines appear wavy. There is a decrease in the brightness of colours and difficulty in discriminating between shades of light and dark. Whereas most of us adapt quickly from light to dim illumination, AMD sufferers take much longer. Blurred vision together with the presence of blind spots makes it very difficult to read or recognise faces, generally diminishing the quality of later life.
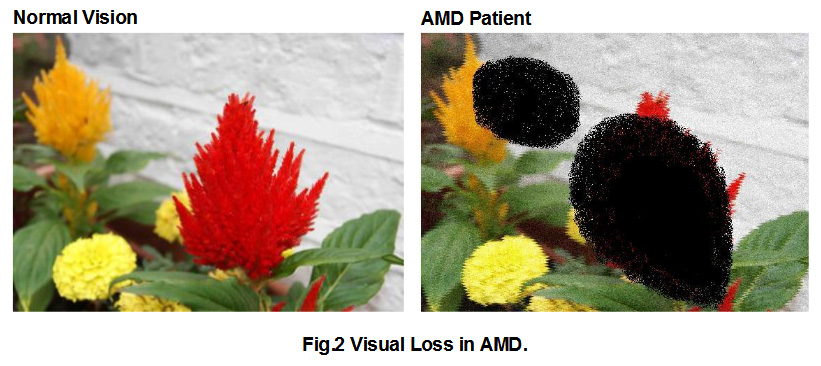
The Amsler grid (Fig.1) is used as a preliminary diagnostic test for AMD. Patients are asked to look at the central spot and describe the shape of the horizontal and vertical lines. Depending on the stage of the disease, patients either describe wavy curvatures in certain regions and blind spots where the lines are missing (Fig.1). The corresponding effects on their visual fields are depicted in Figure 2.
Currently there is NO TREATMENT for AMD. Patients are simply advised to minimise the risk factors associated with AMD. These include stopping smoking, managing high cholesterol and blood pressure, reducing exposure to bright lights and taking nutritional supplements high in anti-oxidants. About 10% of AMD patients develop secondary complications that lead to formation and leakage from new blood vessels and this can cause sudden loss of vision. Anti-VEGF drugs now manage these complications effectively but this intervention does not alter the underlying progression of the disease.
Recent advances in research have provided a better understanding of the mechanisms underlying the development of AMD. It appears that the normal ageing process within the eye is considerably accelerated in AMD leading to the death of the visual cells of the retina.
For effective therapeutic intervention, the metabolic support to the retina needs to be improved. Scientists at AltRegen have demonstrated that compounds in saponin extract can significantly improve the delivery pathways for providing nutritional support to the retina. Such an intervention is expected to slow the ageing process and thereby prevent the degenerative progress of AMD. This is the first viable treatment procedure for the prevention and treatment of AMD.
Anatomy and physiology of vision
Gross anatomy and physiology of the eye
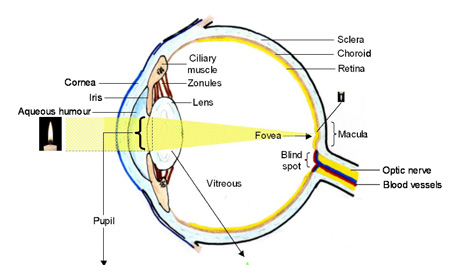
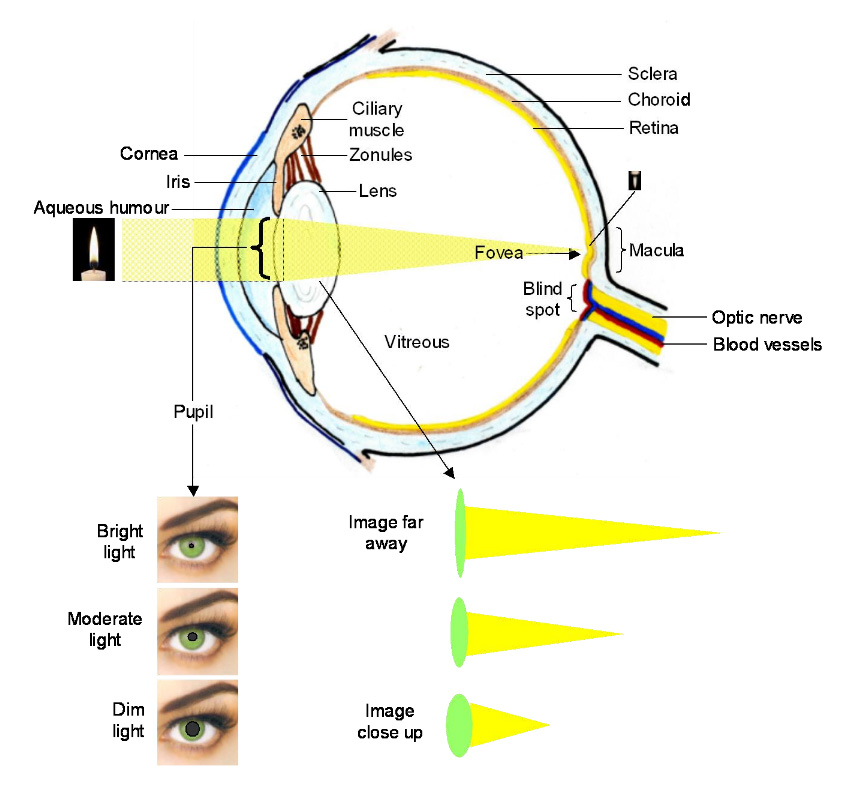
Light from an object, such as the candle in the figure, is focused primarily by the curvature of the cornea. The lens can modulate this focusing slightly to ensure that a clear image (that is inverted) falls on the back of the eye.
The amount of light entering the eye is controlled by the size of the pupil. Too much light can damage the retina and also lead to momentary "blindness". For example, after looking at the sun, it is difficult to image the surroundings for a few seconds. Thus in bright illumination, the pupil is highly constricted. In low light conditions, such as moonlight, the pupil is fully open to allow detection of very small amounts of light stimuli.
Although the major focusing of the image is undertaken by the cornea, changes in the shape of the lens, mediated by the ciliary muscles, can fine tune the degree of focus so that a sharp image lands on the retina. When viewing far objects, the lens is much thinner. It is more relaxed taking on a spherical shape when viewing objects closer to the eye. This ability to alter shape is diminished as we get older, a condition referred to as presbyopia.
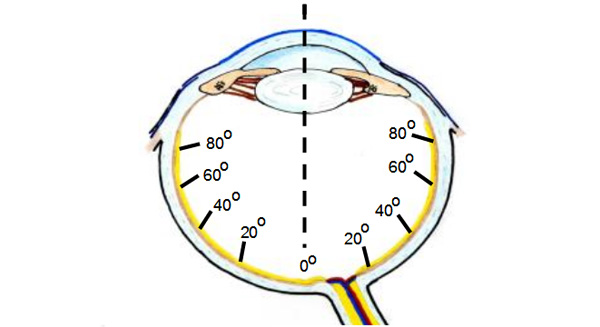
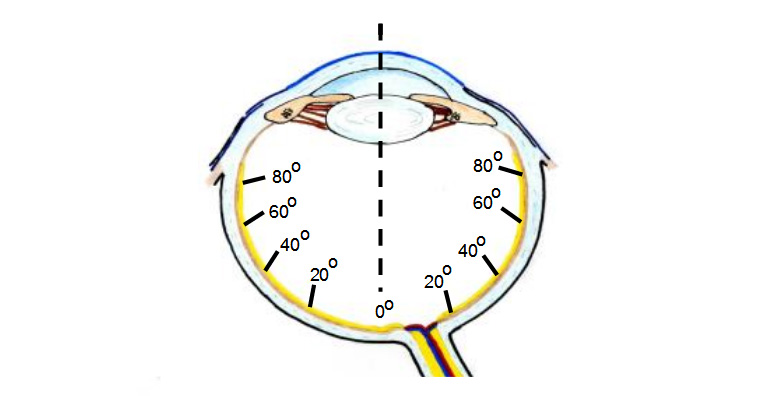
The retina is the light sensitive tissue of the eye and covers nearly two-thirds of the inner globe. Under normal daylight conditions, the focused image is placed in the macular region at the back of the eye. This region occupies only 2% of the retinal surface but is responsible for delivering all our visual awareness. Even at night, a light flash may fall on the peripheral retina, but the eye is automatically re-directed to the source so that the next image falls on the macula for greater scrutiny.
The information within the image gathered by the retina is taken out of the eye via the optic nerve through an opening in the sclera at the back of the globe. Since the optic nerve head (called the optic disc) is devoid of retinal cover, any image falling on this region will not be detected. This region is therefore known as the blind spot. You can find this blind spot in your own eye by looking at Figure 4.
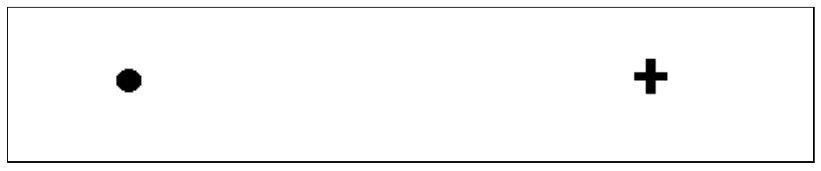
Look at the figure with your head about 20 inches from the screen. Close your right eye. With your left eye, look at the cross. Slowly bring your head closer to the screen whilst keeping fixed on the cross. At a certain distance, the dot will disappear from sight because its image has fallen on your blind spot.
Structure and function of the retina
1. The fundus of the eye
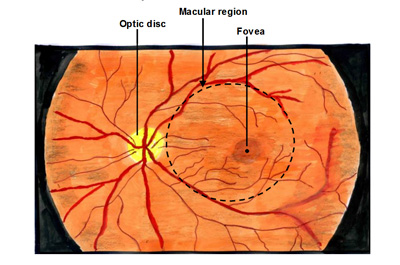
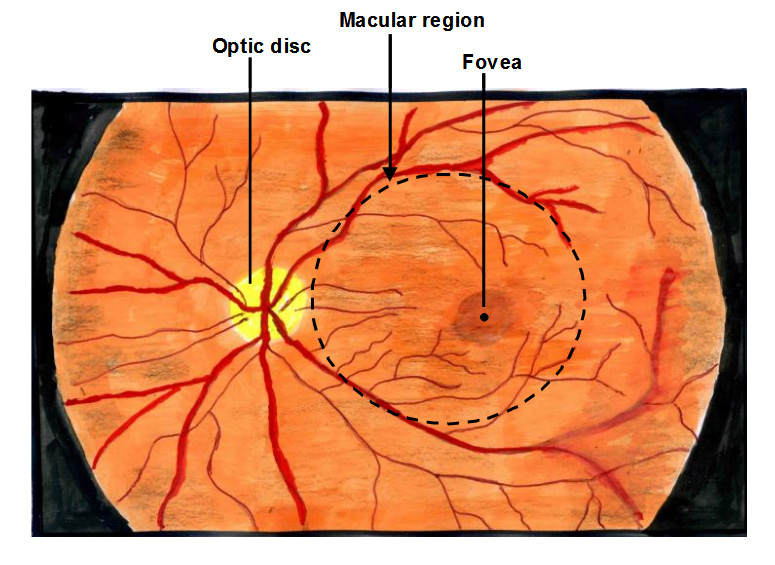
An ophthalmscope is used to view the back of a living eye and the typical features in the macular region of a normal eye are illustrated in the figure. A circular pale yellowish disc is the site of exit of the optic nerve. The blood vessels that supply two-thirds of the retina enter the eye through the optic disc and spread both on the surface and through the structure of the retina.
The macular region (shown as a dashed circular region) lies within the superior and inferior blood vessel "arcades". Within the macular region is a slightly depressed dark spot known as the fovea; this houses the highest density of photoreceptors and is used for discriminating fine detail.
2. Retinal structure
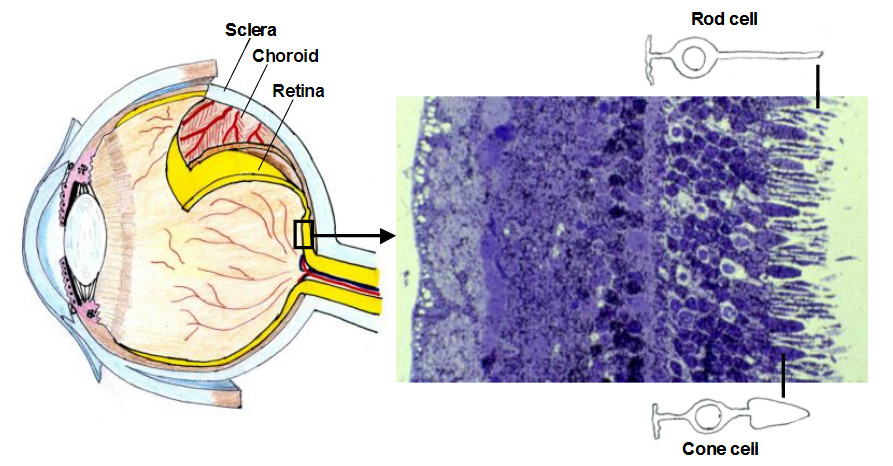
Different layers of tissue lining the globe can be peeled away as shown in the figure. The thickest of these is the sclera and provides mechanical support to the eye. Lying on top of the sclera is the choroid, a tissue complex saturated with blood vessels providing metabolic support to the photoreceptor cells of the retina.
The retina is the innermost layer lining the inside of the eye and an enlarged, blue stained section is shown on the right in the figure. When isolated from a dark-adapted eye, the inner retina is transparent (allowing the transmission of light through it) whereas the outermost region is pinkish in colour due to the presence of the photopigment, rhodopsin.
Retinal nutrition is provided by a dual blood supply. The inner retina is supplied by blood vessels coming out of the optic disc and spreading on the surface and within the inner region. However, photoreceptors are supplied by the blood circulation in the choroid.
3. Rod and cone cells and information transfer in the retina
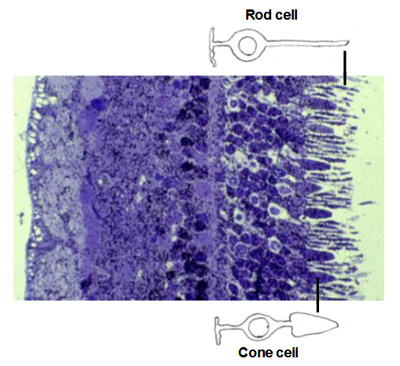
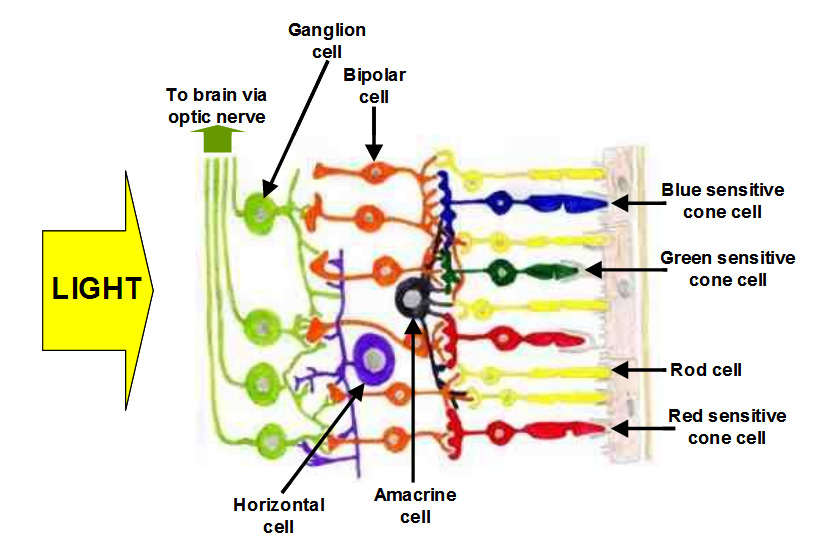
Rod and cone cells and information transfer in the retina. Light is detected by the photoreceptors and the information is passed on to other retinal cells in the inner retina for processing and final transmission via the optic nerve to the brain. There are essentially two types of photoreceptor cells, rods and cones, so named because of the shape of their light detection apparatus. In the human eye, there are about 120 million rods and 6-7 million cone cells.
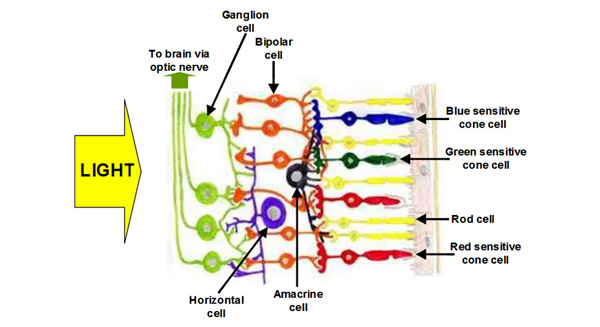
Rod cells function optimally when light levels are low such as at night. As light levels increase, these cells become saturated and cannot contribute to visual function. Cone cells on the other hand operate in moderate to bright light and are therefore responsible for daylight vision. The intensity of light detected by rod or cone cells is transmitted to bipolar cells and these in turn pass on the information to the ganglion cells. However this basic information is processed by horizontal and amacrine cells so that not only is the detection of light by a given cell is registered but the amount of light in neighbouring cells is also included. The final signal sent to the brain is therefore very complicated but contains sufficient information for us to visualise our surroundings.
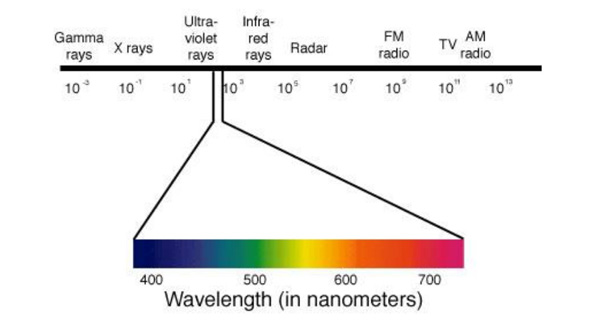
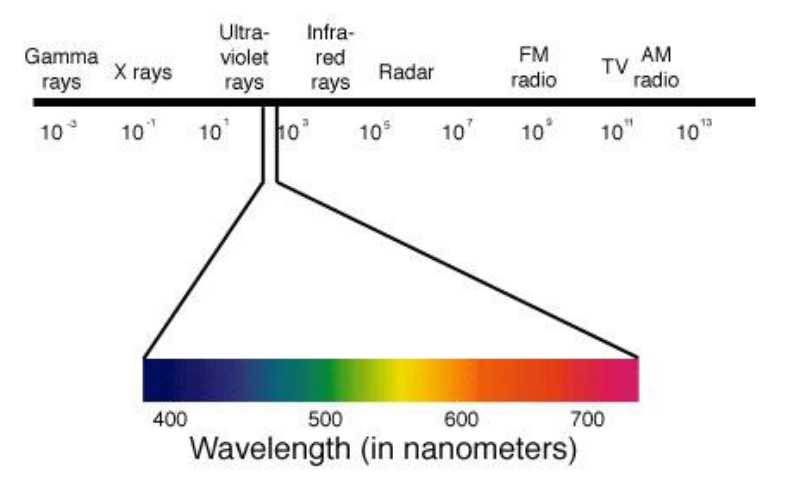
There are several types of cone cells, some responding to a limited range of wavelengths and others acting as motion detectors. The three major types are divided into red-, green-, or blue sensitive cones depending on the maximal absorption wavelength of light. In combination therefore, these cells allow us to appreciate the colours of the whole visual spectrum between 400-700nm.
4. Clarity of the visual image
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
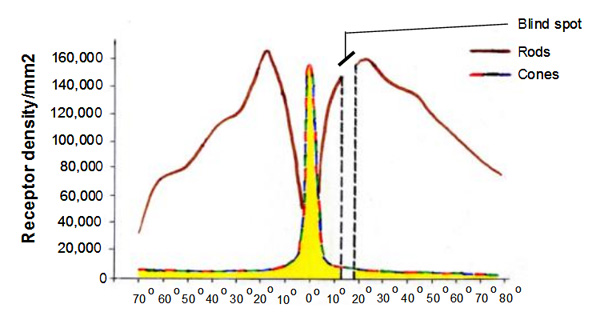
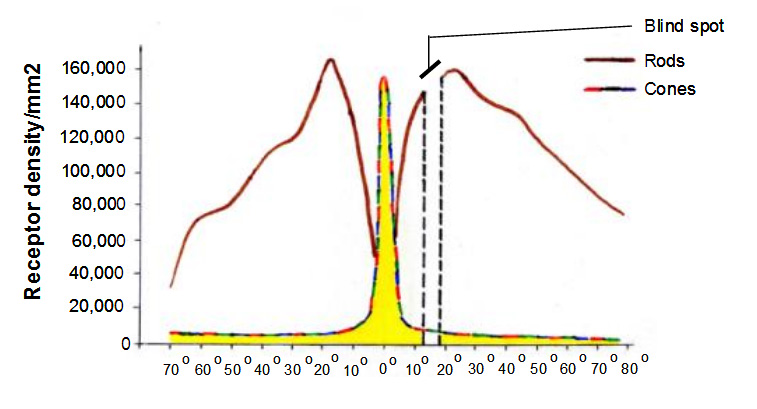
In a digital camera, the resolution of the captured image is dependent on the pixel density of the detector. This is also true in the eye. If we know the density of photoreceptors in the eye, we can find the region that provides the greatest resolution. In the diagram below, the highest density of cone photoreceptor cells in found within the fovea, the region of highest resolution for daylight vision. The highest density of rod photoreceptors is also found in the macular region. Rod and cone densities fall away outside the macula. Thus in normal lighting conditions, the image obtained by the cornea and lens is focused on the macular region and for close-up work, on the fovea. If you focus on an object in front of you, then the image of the surroundings falls on the peripheral retina and it is very difficult to even recognise faces.
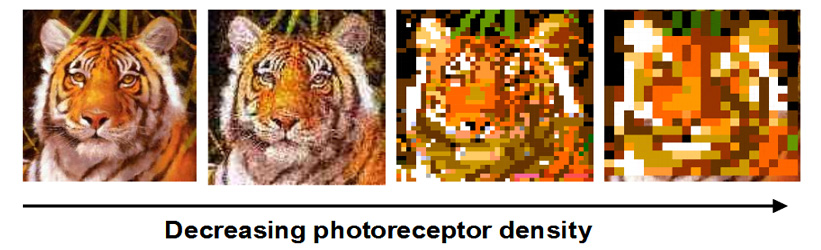
In diseases that lead to death of photoreceptors, the spatial density of these cells falls and therefore the image starts to degrade, commonly described as blurriness of vision. This is illustrated below where progressive loss of photoreceptors leads to blurred and unrecognisable images. In daily life, this would make it very difficult to read text and to recognise familiar faces. Further loss of photoreceptors would lead to blind spots and regions within the visual field of an individual patient.
Age-related Macular Degeneration (AMD) treatment depends on ‘cleaning-up’ Bruch’s membrane
Learn more about AMD
Everything you need to know about Age-related Macular Degeneration.